|
 Yellow
Fever Yellow
Fever
Yellow fever is a viral illness which is spread by the
bite of a mosquito. The species of mosquito that is responsible
for spreading yellow fever is Aedes Aegypti
and is a different species from the anopheles mosquito
that transmits malaria.
Essentially yellow fever is a disease
of monkeys living in tropical rain forests. The virus which
causes the disease is one of a group of viruses known as arboviruses.
Humans are infected by being bitten by rain forest mosquitos
carrying the yellow fever virus.
 As
their name implies "arboviruses" are transmitted to humans
by insects (arthropod borne virus). The mosquito in particular
is well suited to the transport and spread of the infection
due to its wide distribution throughout the tropics. As
their name implies "arboviruses" are transmitted to humans
by insects (arthropod borne virus). The mosquito in particular
is well suited to the transport and spread of the infection
due to its wide distribution throughout the tropics.
The peak biting times for many mosquito species is dusk to
dawn. However, Aedes aegypti that transmits yellow
fever virus, feeds during the daytime.
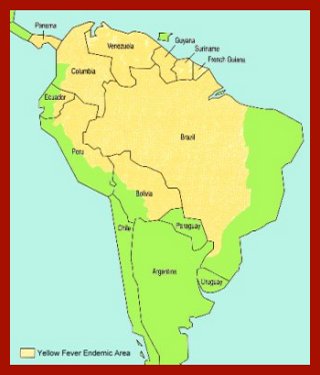
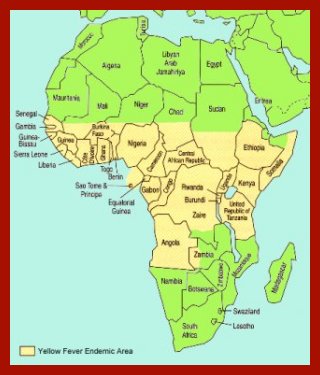 The
geographical distribution of yellow fever is confined
to Equatorial Africa and Central South America as shown on
the maps as shown. The
geographical distribution of yellow fever is confined
to Equatorial Africa and Central South America as shown on
the maps as shown.
Strangely, yellow fever is unknown in Asia despite
the presence of mosquitos capable of spreading the virus.
Arbovirus illnesses
usually have two characteristic phases, the first when the
virus is invading the host cells, and the second a few days
later when the body's immune system is fighting the infection.
The antibodies produced during the second phase of
illness can cause damage to the blood vessels which explains
why arboviruses often cause bleeding.
Many yellow fever infections are mild and go unrecognised
but severe and life threatening illness is not uncommon. After
an incubation period of about three to six days fever, headache,
abdominal pain and vomiting develop. After a brief recovery
period, shock, bleeding and signs of liver and kidney failure
develop. Liver failure is associated with jaundice hence the
name "yellow fever".
There are no drugs available
to cure yellow fever hence treatment is aimed at symptomatic
relief. Overall about 5% of patients die. Those who recover
do so completely and are immune thereafter.
Fortunately yellow fever is
one of the few arboviruses for which a vaccination is available.
A single injection of a live, weakened (and harmless) virus
stimulates the body's immune defences and confers effective
immunity for ten years.
| For
a list of clinics in the UK where you can obtain yellow
fever & other vaccines:- |
| |
|
|
 |
|
In
general, all travellers going to an endemic area require
a yellow fever vaccination certificate and travellers
going to some parts of Asia from an endemic region will
also require a certificate.
|
 Dengue
Fever Dengue
Fever
This is an unusual arbovirus infection
since no other animals except humans and mosquitoes play a
significant part in perpetuating the infection. It is present
in Africa, South East Asia, the Pacific area and northern
South America.
The disease is spread to humans by the bite of a mosquito
(Aedes aegypti) and after about five days incubation
period there is a sudden onset of fever, headache and severe
joint and muscle pains. The initial fever resolves after about
three to five days only to recur with the appearance of a
rash consisting of small white spots which starts on the trunk
and spreads to the limbs and face. Within a few days the fever
subsides and recovery follows.
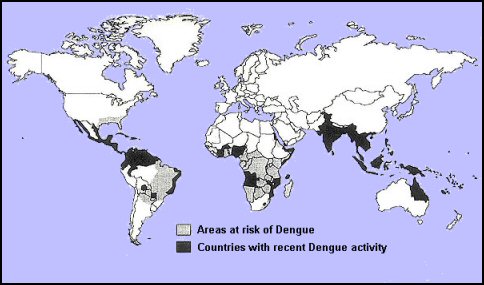
Dengue is the second most commonly identified cause of fever
in unwell international travellers.It is widespread throughout
the tropics and subtropics, occurring in more than 120 countries.
Outbreaks due to imported infection have recently been reported
in Southern Europe.
Outbreaks of dengue are common and often occur in a seasonal
pattern. Nearly 100 million cases of dengue are thought to
occur every year. Severe infection mainly affects infants
and children living in the tropics and subtropics.
 Dengue
is caused by any one of four related viruses transmitted
by mosquitoes. Currently the most effective protective measures
are those that avoid mosquito bites. Dengue
is caused by any one of four related viruses transmitted
by mosquitoes. Currently the most effective protective measures
are those that avoid mosquito bites.
When infected, early recognition and prompt supportive
treatment can substantially lower the risk of medical complications
and death.
There is no specific treatment for Dengue but in terms
of management, sufferers are advised to take paracetamol and
oral rehydration.
Although dengue is a very unpleasant illness, complications
are uncommon and recovery is usually complete.
 There is also a more severe and life threatening haemorrhagic
form of the disease which has appeared with dramatic outbreaks.
Fortunately this form occurs only rarely.
There is also a more severe and life threatening haemorrhagic
form of the disease which has appeared with dramatic outbreaks.
Fortunately this form occurs only rarely.
This is thought to be the result of a second infection
where there is some remaining immunity from a first attack
causing a vigorous immunological response in which severe
blood vessel damage occurs.
Unfortunately, immunity to infection does not last
long and subsequent attacks are possible. Prevention is mainly
by avoiding mosquito bites. However, a vaccine is now available.
Note: The Aedes mosquito responsible for transmitting Dengue
Fever is a day time feeding species.
A dengue
fever vaccine called Qdenga® is now licenced for use
in the UK.
The vaccine
is only recommended for some travellers that have already
been infected with Dengue in the past. If
you are considering getting vaccinated you should arrange
a travel health consultation to discuss if the Dengue vaccine
is suitable for you.
World's
first vaccine against the Dengue virus
was approved in Mexico |
|
The
first vaccine to prevent dengue fever has been approved
for use in Mexico by the country’s drugs regulator.
The decision by the Federal Commission for the Protection
against Sanitary Risk (COFEPRIS) was based on the results
of more than 25 clinical trials conducted by vaccine
manufacturer Sanofi Pasteur in 15 countries – including
Mexico – which involved more than 40,000 volunteers.
Dengvaxia is a vaccine developed for prevention
of disease caused by all four dengue virus serotypes
and is made from attenuated dengue. The product is authorised
for use in populations where dengue is endemic.
COFEPRIS says the vaccine has an average efficacy of
60% for preventing infection and 93% efficacy for preventing
severe dengue infection in patients aged 9–45 years.
Estimates are that the vaccine could help prevent 8,000
hospital admissions and 104 deaths every year from the
virus in Mexico, saving 1,100 million pesos in healthcare
costs. In 2014, Mexico recorded 32,100 cases of dengue
fever.
Manufacturer Sanofi Pasteur, has spent more than 20
years developing a vaccine. The company claims it has
the potential to reduce cases of dengue fever by 50%
within five years in populations where the disease is
endemic.
Dengvaxia is the first vaccine approved to prevent dengue
fever and is a major innovation and a public health
breakthrough. It will be a critical addition to the
integrated dengue prevention and control efforts.
|
 Japanese
B Encephalitis Japanese
B Encephalitis
This is a rare
but serious arboviral infection with a 20% fatality rate.
It occurs in most of the Far East and South East Asia. The
endemic zone extends from India and Nepal across the whole
of South East Asia to Japan and Korea in the Far East.
The risk of infection is greatest in long term visitors
to rural areas, and the risk to short term visitors and visitors
to major cities is small. Precautions against mosquito bites
are essential.
Japanese B Encephalitis is transmitted by rice field
breeding mosquitoes (of the Culex group) that become infected
with Japanese encephalitis virus.
 Mosquitoes
become infected by feeding on domestic pigs and wild birds
infected with the Japanese encephalitis virus. Infected mosquitoes
then transmit the Japanese encephalitis virus to humans and
animals during the feeding process. Mosquitoes
become infected by feeding on domestic pigs and wild birds
infected with the Japanese encephalitis virus. Infected mosquitoes
then transmit the Japanese encephalitis virus to humans and
animals during the feeding process.
The incubation period is normally between 5 and 15 days.
The illness cannot be passed on from person to person.
There is no specific treatment. Intensive supportive therapy
is indicated.
Mild infections can sometimes
occur without apparent symptoms other than mild fever
with headache. More severe infection is marked by quick onset,
headache, high fever, neck stiffness, stupor, disorientation,
coma, tremors, occasional convulsions (especially in infants)
and spastic paralysis.
There is an effective vaccine
available in the UK on a named patient basis. It should
be considered by anyone travelling to south and sotheast Asia
for more than a month or visiting rural areas.
 Tick
Borne Encephalitis Tick
Borne Encephalitis
Ticks are
blood feeding external parasites of mammals, birds, and reptiles
throughout the world. Ticks are not insects like fleas, but
arachnids like mites, spiders and scorpions.
Tick-borne
encephalitis (TBE), is a viral disease affecting the central
nervous system. The disease is most often manifest as meningitis
or encephalitis or sometimes, even meningoencephalitis. It
is caused by the tick-borne encephalitis virus (TBEV), a member
of the family Flaviviridae.
TBE
is endemic in many European countries, the former Soviet Union,
and Asia. It is found mainly in temperate regions. The natural
hosts of the virus are small rodents and deer, with humans
being accidental hosts. After attaching itself to the host,
an infected tick transfers the virus to the host during feeding.
In disease
endemic areas, people with recreational or occupational exposure
to rural or outdoor settings such as; hunters, hikers, campers,
forest workers, farmers, etc. are potentially at risk of infection
by contact with the infected ticks.
The incubation period of TBE is usually between 7 and 14 days.

Map
showing TBE endemic areas
A characteristic
biphasic febrile illness follows, with an initial phase that
lasts two to four days. It is non-specific with symptoms that
may include fever, malaise, anorexia, muscle aches, headache,
nausea, and/or vomiting.
 After
about eight days of remission, the second phase of the disease
occurs in twenty to thirty percent of patients and involves
the central nervous system with symptoms of meningitis (fever,
headache, and a stiff neck) or encephalitis (drowsiness, confusion,
sensory disturbances, and/or motor abnormalities such as paralysis)
or meningoencephalitis. TBE is more severe in adults than
in children. After
about eight days of remission, the second phase of the disease
occurs in twenty to thirty percent of patients and involves
the central nervous system with symptoms of meningitis (fever,
headache, and a stiff neck) or encephalitis (drowsiness, confusion,
sensory disturbances, and/or motor abnormalities such as paralysis)
or meningoencephalitis. TBE is more severe in adults than
in children.
 Mortality
is about two percent with deaths occurring five to seven days
after the onset of neurological signs. Mortality
is about two percent with deaths occurring five to seven days
after the onset of neurological signs.
There
is no specific treatment for TBE. Meningitis, encephalitis,
or meningoencephalitis require hospitalisation and supportive
care.
Like other tick-borne infectious diseases, TBEV infection
can be prevented by using insect repellents and protective
clothing to prevent tick bites.
A vaccine is available in some disease endemic areas but adverse
vaccine reactions in children limit the use of the vaccine.
The vaccine involves two doses one month apart. If required
a booster is given after a year.
| Symptoms
of West Nile Virus |
- symptoms
of a mild infection: fever, headache, bodyaches,
skin rash, and swollen lymph glands
- symptoms
of a severe infection may be marked by: high fever,
severe headache, neck stiffness, stupor, disorientation,
tremors, convulsions, muscle weakness, paralysis,
and coma
- Contact
your health care provider if you have concerns about
your health. If severe symptoms develop, see your
doctor immediately.
|
West
Nile Virus
West Nile Virus is a flavivirus commonly found in Africa, West
Asia, the Middle East and the United States. The virus can infect
humans, birds, mosquitoes, horses and some other mammals.
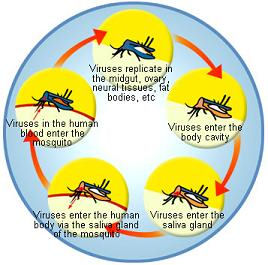
The principal route of human infection with West Nile virus
is through the bite of an infected mosquito. Mosquitoes become
infected when they feed on infected birds, which circulate the
virus in their blood for a few days. The virus replicates in
the mosquito and spreads to the mosquito's salivary glands.
During subsequent blood meals, the virus may be injected into
humans and animals, where it can multiply and possibly cause
illness.
At least 36 species of mosquito are known to be carriers of
West Nile Virus. The most common carrier of West Nile in the
United States is the Culex pipiens (Northern house) mosquito.
 West
Nile fever is usually a case of mild disease characterized
by flu-like symptoms. It typically lasts only a few days and
does not appear to cause any long-term health effects. West
Nile fever is usually a case of mild disease characterized
by flu-like symptoms. It typically lasts only a few days and
does not appear to cause any long-term health effects.
More severe disease due to a person being infected with this
virus can be West Nile encephalitis, West Nile meningitis
or West Nile meningoencephalitis. Encephalitis refers to an
inflammation of the brain, meningitis is an inflammation of
the membrane around the brain and the spinal cord, and meningoencephalitis
refers to inflammation of the brain and the membrane surrounding
it.
The incubation period is usually 3 to 14 days. Symptoms of
mild disease will generally last a few days. Symptoms of severe
disease may last several weeks, although neurological effects
may be permanent.
Many people
who are infected with the West Nile virus will not have any
type of illness. It is estimated that 20% of the people who
become infected will develop West Nile fever: mild symptoms,
including fever, headache, and body aches, occasionally with
a skin rash on the trunk of the body and swollen lymph glands.
 The
symptoms of severe infection (West Nile encephalitis or meningitis)
include headache, high fever, neck stiffness, stupor, disorientation,
coma, tremors, convulsions, muscle weakness, and paralysis.
It is estimated that 1 in 150 persons infected with the West
Nile virus will develop a more severe form of disease. The
symptoms of severe infection (West Nile encephalitis or meningitis)
include headache, high fever, neck stiffness, stupor, disorientation,
coma, tremors, convulsions, muscle weakness, and paralysis.
It is estimated that 1 in 150 persons infected with the West
Nile virus will develop a more severe form of disease.
There is no specific treatment for West Nile virus infection.
In more severe cases, intensive supportive therapy is indicated,
often involving hospitalization, intravenous fluids, airway
management, respiratory support (ventilator), prevention of
secondary infections (pneumonia, urinary tract, etc.), and
good nursing care.
When travelling to areas where the disease is endemic you
can reduce the risk of becoming infected with the virus by
employing preventive measures such as protecting yourself
from mosquito bites:-
- Apply
insect rellent to your skin and clothes when going
outside
- When
possible, wear long-sleeved shirts and long pants
whenever you are outdoors.
- Place
mosquito netting over infant carriers when you are
outdoors with infants.
- Consider
staying indoors at dawn, dusk, and in the early evening,
which are peak mosquito biting times.
- Make
sure any window and door screens are intact so that
mosquitoes cannot get indoors.
- Use
mosquito nets around beds at night while asleep.
|
 Many
of the mosquitoes that carry the West Nile virus are especially
likely to bite around dusk and dawn. If you are outdoors around
these times of the day, it is important to apply repellent.
But there are also mosquitoes that bite during the day, and
these mosquitoes have also been found to carry the West Nile
virus. The safest decision is to apply repellent whenever
you are outdoors Many
of the mosquitoes that carry the West Nile virus are especially
likely to bite around dusk and dawn. If you are outdoors around
these times of the day, it is important to apply repellent.
But there are also mosquitoes that bite during the day, and
these mosquitoes have also been found to carry the West Nile
virus. The safest decision is to apply repellent whenever
you are outdoors
 Apply
insect repellent sparingly to exposed skin. The more DEET
a repellent contains the longer time it can protect you from
mosquito bites. A higher percentage of DEET in a repellent
does not mean that your protection is betterjust that it
will last longer. DEET concentrations higher than 50% do not
increase the length of protection. Apply
insect repellent sparingly to exposed skin. The more DEET
a repellent contains the longer time it can protect you from
mosquito bites. A higher percentage of DEET in a repellent
does not mean that your protection is betterjust that it
will last longer. DEET concentrations higher than 50% do not
increase the length of protection.
Choose a repellent that provides protection for the amount
of time that you will be outdoors.
 Chikungunya
fever Chikungunya
fever
Chikungunya fever is another viral disease transmitted
to humans by the bite of infected mosquitoes. It is diagnosed
based on symptoms, physical findings (e.g., joint swelling),
laboratory testing, and the possibility of exposure to infected
mosquitoes.
Chikungunya typically starts with one or more of the following
symptoms - chills, fever, vomiting, nausea, head ache and
joint pain. The attack is sudden and sometimes it is accompanied
with rashes. Severe joint pain is the main and the most problematic
symptom of Chikungunya.
Other
less commonly seen symptoms include mouth ulcers, loss
of taste and conjunctivitis. The fever usually subsides in
a couple of days, but other symptoms may last for a longer
duration. In some cases joint pain persisted for years.
There is no antiviral drug or medicine specifically
for Chikungunya fever; care is based on symptoms. Chikungunya
infection is not usually fatal and since chikungunya is cured
by the immune system in almost all cases there is no need
to worry.
Steps to prevent infection with chikungunya virus include
use of insect repellent, protective clothing, and staying
in areas with screens.
Chikungunya virus was first isolated in Tanzania in
1953, and has since been cited as the cause of numerous human
epidemics in India, Indonesia, Malaysia, Singapore, and Sri
Lanka.

Chikungunya Distribution and Global Map
The
geographic range of chikungunya virus is mainly in Africa
and Asia. Given the current large chikungunya virus epidemics
and the worldwide distribution of Aedes aegypti and
Aedes albopictus mosquitoes, there is a risk of importing
chikungunya virus into new areas through infected travellers.
|
Countries
where people have become infected with Chikungunya virus
|
| Benin |
Guinea |
Maldives
|
Singapore |
| Burundi |
India |
Mauritius |
South
Africa |
| Cambodia |
Indonesia |
Mayotte |
Sudan |
| Cameroon |
Italy |
Myanmar |
Taiwan |
| Central
African Republic |
Kenya |
Nigeria |
Tanzania |
| Comoros |
Laos |
Pakistan |
Thailand |
| Congo |
Madagascar |
Philippines |
Uganda |
| East
Timor |
Malawi |
Senegal |
Vietnam |
| Equatorial
Guinea |
Malaysia |
Seychelles |
Zimbabwe |
Zika
Virus
 If
you’ve heard about the Zika virus
and are wondering what it is, you’re not alone. Cases
of this emerging infectious disease are soaring in the Americas
and "spreading explosively," according to World
Health Organization Director-General Margaret Chan, MD. Several
states are reporting cases of U.S. travelers bringing the
infection back with them, and health officials in Texas have
confirmed a case of sexual transmission of the virus. If
you’ve heard about the Zika virus
and are wondering what it is, you’re not alone. Cases
of this emerging infectious disease are soaring in the Americas
and "spreading explosively," according to World
Health Organization Director-General Margaret Chan, MD. Several
states are reporting cases of U.S. travelers bringing the
infection back with them, and health officials in Texas have
confirmed a case of sexual transmission of the virus.
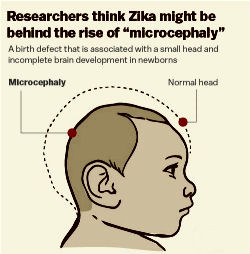
For
most people,
the Zika virus causes only a brief, mild flu-like illness.
But in pregnant women it has been linked to an alarming increase
in the rate of the birth defect known as microcephaly —
a debilitatingly small head and brain size. The clusters of
birth defects linked to the Zika virus are an international
public health emergency, according to the WHO. Dr. Chan characterizes
the situation as an "extraordinary event and a public
health threat to other parts of the world."
The Centers for Disease Control and Prevention in the
USA posted a travel alert advising pregnant women to delay
travel to areas where Zika is active. The travel alert list
continues to expand and now includes 28 countries or territories,
most of them in the Americas.
 The
CDC's newest guidelines recommend that pregnant women
coming back from these areas get tested for Zika if they have
symptoms. The
CDC's newest guidelines recommend that pregnant women
coming back from these areas get tested for Zika if they have
symptoms.
The
World Health Organization
expects Zika to spread to all but two countries in the Americas:
Canada and Chile.
The
most common symptoms of Zika virus disease are fever,
rash, joint pain, and conjunctivitis. The illness is usually
mild with symptoms lasting from several days to a week. Severe
disease requiring hospitalization is uncommon.
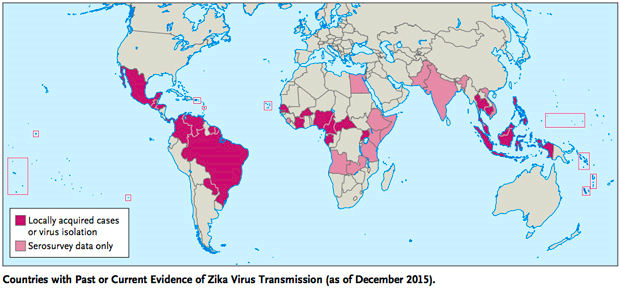
Outbreaks
of Zika have occurred in areas of Africa, Southeast Asia,
the Pacific Islands, and the Americas. Because the Aedes species
mosquitoes that spread Zika virus are found throughout the
world, it is likely that outbreaks will spread to new countries.
In December 2015, Puerto Rico reported its first confirmed
Zika virus case. Locally transmitted Zika has not been reported
elsewhere in the United States, but cases of Zika have been
reported in returning travelers.
 There
is no vaccine to prevent or medicine to treat Zika. Travellers
can protect themselves from this disease by taking anti-mosquito
measures: When traveling to countries where Zika virus has
been reported, use insect repellents, wear long sleeves and
pants, and stay in places with air conditioning or that have
window and door screens. There
is no vaccine to prevent or medicine to treat Zika. Travellers
can protect themselves from this disease by taking anti-mosquito
measures: When traveling to countries where Zika virus has
been reported, use insect repellents, wear long sleeves and
pants, and stay in places with air conditioning or that have
window and door screens.
Zika virus can be spread from a pregnant woman to her unborn
baby. There have been reports of a serious birth defect of
the brain called microcephaly and other poor pregnancy outcomes
in babies of mothers who were infected with Zika virus while
pregnant.
Knowledge of the link between Zika and these outcomes is evolving,
but special precautions are recommended for the following
groups:
-
Women
who are pregnant (in any trimester): Consider postponing
travel to any area where Zika virus transmission is ongoing.
If you must travel to one of these areas, talk to your
doctor first and strictly follow steps to prevent mosquito
bites during your trip.
-
Women
who are trying to become pregnant: Before you travel,
talk to your doctor about your plans to become pregnant
and the risk of Zika virus infection. Strictly follow
steps to prevent mosquito bites during your trip.
|
10
Facts about the Zika Virus
|
-
The
Zika virus is carried by mosquitoes and people,
but usually spread by mosquitoes.
-
Symptoms
of Zika virus infection are usually mild.
-
Unborn
babies are most at risk from Zika virus complications.
-
There
are no vaccines at present to protect against the
Zika virus.
-
Zika
began in Africa and spread rapidly.
-
Zika
has reached Puerto Rico’s mosquitoes and may
keep traveling north.
-
U.S.
travellers are taking the viral disease back into
the USA with them. Which means other nationalities
can too.
-
Travelers
are unlikely to bring infected mosquitoes along
with them.
-
You
can help prevent Zika infection by using insect
repellents.
-
Mosquito
control can help prevent Zika.
|
|


 Arboviruses
are viruses transmitted to humans by arthropods such as
mosquitoes and ticks. The first two letters of the words arthropod'
and borne, make up the 'arbo' that now designates this group
of viruses as arthropod-borne:
Arboviruses
are viruses transmitted to humans by arthropods such as
mosquitoes and ticks. The first two letters of the words arthropod'
and borne, make up the 'arbo' that now designates this group
of viruses as arthropod-borne: The
way to prevent arboviruses is simply by avoiding the vectors
that carry them, but protecting yourself is also important.
The
way to prevent arboviruses is simply by avoiding the vectors
that carry them, but protecting yourself is also important.