A
key to the abbreviations used and information on the different
anti-malarial drug regimens can be found below the main
tables
Malaria
endemic countries in Asia & Middle East Note:
In this map, countries with areas endemic for malaria are shaded
completely even if transmission occurs
in only part of that country. For more specific within country
information, see the guidelines below.
Dengue
Risk in Asia & Middle East
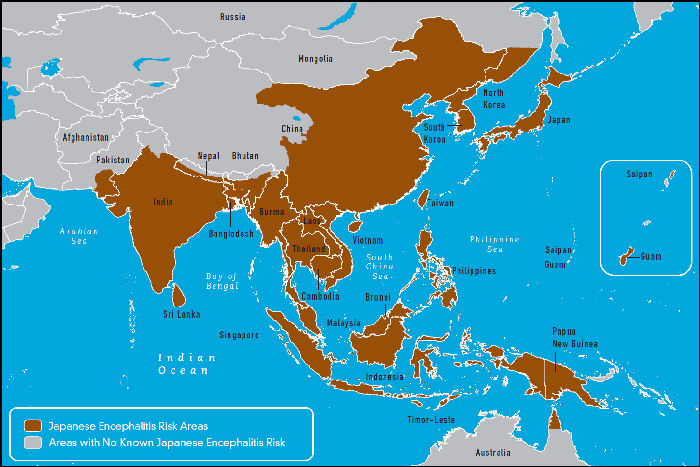
Geographic
Distribution of Japanese Encephalitis
Disease
Risks in the Indian Subcontinent
Bangladesh,
Bhutan, India, Maldives, Nepal, Pakistan, Sri Lanka.
Borneo
(see Indonesia and Malaysia), Brunei Darussalam, Burma (see
Myanmar), Cambodia, China (including Tibet), East Timor, Hong
Kong (see China), Indonesia (including Bali and southern Borneo),
Japan, Korea, Laos, Macao (see China), Malaysia (Peninsular
Malaysia and northern Borneo, including Sarawak and Sabah),
Mongolia, Myanmar (formerly Burma), the Philippines, Singapore,
Taiwan, Thailand, Tibet (see China), Vietnam.
Vaccination is mandatory
and a certificate of vaccination is required for
entry.
C
A certificate
of vaccination may be required if entering from
an endemic country, (except for children <1 year
old).
R
Vaccination is recommended
for the country but no evidence is required for
entry.
L
Long Term. Vaccination
recommended for travellers staying in endemic
areas for 3 months or more. Except Japanese B
Encephalitis if longer than 1 month.
COUNTRY
MALARIA
REGIMEN
YEL
HEP
A
TYP
TET
POL
MEN
ENC
DIP
RAB
HEP
B
Afghanistan Malaria risk below 2000
metres from May to Nov
2
C
R
R
R
R
-
-
L
L
L
Armenia Malaria risk in some
villages in the Ararat Valley, mainly in the Masis
district, from June to October - Regimen 3. No
risk in the main tourist areas Regimen 4.
3/4
-
R
R
R
R
-
-
L
L
L
Azerbaijan Limited malaria risk
from June to October in the south border area
and Khachmas. Also in lowland areas, mainly in
the areas between the Kura and the Arax rivers.
3
-
R
R
R
R
-
-
L
L
L
Bahrain No malaria risk
-
-
R
R
R
R
-
-
L
L
L
Bangladesh High malaria risk in
the south east and Chittagong Hill Tracts - Regimen
1. All other areas - Regimen 2.
No risk in Dhaka city - Regimen 4.
1/2/4
-
R
R
R
R
-
L
L
L
L
Bhutan Risk of Malaria
is only present in the southern districts of Bhutan.
2
C
R
R
R
R
R
-
L
L
L
Brunei No malaria risk
-
C
R
R
R
R
-
L
L
L
L
Cambodia Malaria risk is present
throughout the country including the areas around
the famous temple complex of Angkor Wat near Siem
Reap - Regimen 1.
Risk
is minimal in the capital city Phnom
Penh, the nearby Mekong river
delta and in the rice growing areas around the
large inland lake of Tonle Sap - Regimen 4.
Note: There is mefloquine resistance present in
western provinces & the border with Thailand.
1/4
C
R
R
R
R
-
L
L
L
L
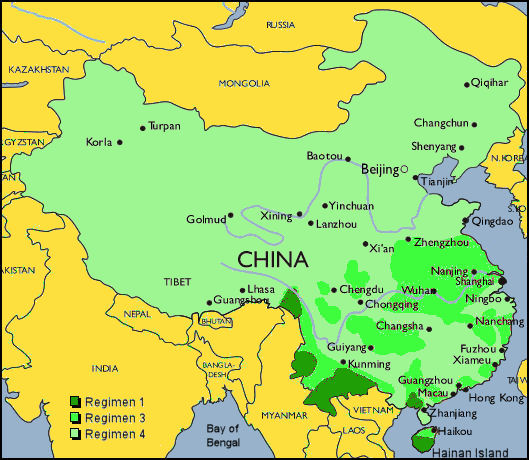
China Urban and densely populated
areas are normally malaria free.
Serious risk of malaria in China is now confined
to a few areas not normally visited by package
tourists or business travellers but may be visited
by backpackers or voluntary workers.
Risk
is present only on Hainan island, in Yunnan province
and sporadically in Guangxi province - Regimen
1.
Less
serious malaria risk occurs in a few isolated
areas in the 'flood' plains of the Yangtze (Chang
Jiang) and Yellow (Huang He) rivers - specifically
within the provinces of
Fujian, Guangxi, Guangdong, Guizhou, Sichuan and
Xizang (along the valley of the Zangbo river).
Isolated
cases occasionally occur in other parts of the
country Regimen 3.
All other regions including the main tourist areas
- very little risk, avoid mosquito bites - Regimen
4.
Georgia Malaria risk in some
areas located in the south eastern part of the
country from July to October.
3
-
R
R
R
R
-
-
R
L
L
Hong
Kong Very low malaria risk
- avoid mosquito bites.
4
C
R
R
R
R
-
L
L
L
L
India Malaria risk exists in
all Indian states below 2000m especially in rural
areas and Goa particularly areas north of Panaji
- Regimen 2. - See note on Goa
Low risk in the southern states of Kerala, Tamil
Nadu, Karnataka, and southern Andhra Pradesh including
Hyderabad and the city of Mumbai - Regimen 3.
Low risk also in the northern states of Rajasthan,
Uttar Pradesh, Punjab and the cities of Delhi
and Aggra.
In
these low risk areas it may not be necessary to
take antimalarial medication especially if travel
is restricted to urban areas - Regimen 3 or 4.
Very low to no risk in northern mountain states
including the high altitude Himalayan states of
Jammu and Kashmir, Himachal Pradesh and Sikkim
- Regimen 4.
High
risk in the eastern state of Assam where resistance
to chloroquine has been reported - Regimen 1.
Indonesia
including Bali There is a malaria risk
throughout Indonesia all year round but the risk
is small in all large cities like Jakarta and
the tourist resorts on the islands of Bali and
Java - Regimen 4.
Travellers
should be aware that the malaria risk is substantial
in islands close to Bali and Java which may be
visited on excursions e.g. Lombok
and
West Papua (previously Irian Jaya) and East Timor
- Regimen 1
All other areas except cities - Regimen 2.
1/2/4
C
R
R
R
R
-
L
L
L
L
Iran Malaria
risk is minimal in areas north of the Zagros mountains
and in western and south-western regions during
the summer months. A more substantial risk is
present from March to November in the south-eastern
provinces of Sistan - Baluchestan, Hormozgan and
Kerman.
2
-
R
R
R
R
-
-
L
L
L
Iraq Malaria
risk in northern rural areas and Basrah province
in the south from May to November.
2
C
R
R
R
R
-
-
L
L
L
Israel No malaria
risk
-
-
R
R
R
R
-
-
L
L
L
COUNTRY
MALARIA
REGIMEN
YEL
HEP
A
TYP
TET
POL
MEN
ENC
DIP
RAB
HEP
B
Japan No
malaria risk
-
-
-
-
R
R
-
L
L
L
L
Jordan No
malaria risk
-
C
R
R
R
R
-
-
L
L
L
Kazakhstan No
malaria risk
-
C
R
R
R
R
-
-
L
L
L
Korea
(north) No
malaria risk
-
-
R
R
R
R
-
L
L
L
L
Korea (south) No
malaria risk
-
-
R
R
R
R
-
L
L
L
L
Kuwait No
malaria risk
-
-
R
R
R
R
-
-
L
L
L
Kyrgystan No
malaria risk
-
-
R
R
R
R
-
-
L
L
L
Laos Malaria
risk in the whole country - Regimen 1, except Vientiane
- Regimen 4.
1/4
C
R
R
R
R
-
-
L
L
L
Lebanon No
malaria risk
-
C
R
R
R
R
-
-
L
L
L
Malaysia Malaria
precautions are essential.
In western peninsular Malaysia the risk is confined
to the Taman Negara National Park (around and east
of Mount Tahan) and some remote inland forested
areas not normally visited by tourists.
In the eastern Malaysian provinces of Sabah and
Sarawak and on the island of Borneo malaria is widespread
- Regimen 1.
However
coastal urban areas of Sarawak are considered minimal
risk - Regimen 2.
All other areas including Kuala Lumpur, Penang &
the developed tourist areas of the Cameron Highlands
are not normally at risk - regimen 4.
1/2/4
C
R
R
R
R
-
L
L
L
L
Maldives No malaria
risk but always take anti-mosquito bite measures.
4
C
R
R
R
R
-
-
L
L
L
Mongolia No malaria
risk but always take anti-mosquito bite measures.
4
-
R
R
R
R
R
-
L
L
L
Myanmar
(Burma) Malaria
risk is present in all areas below 1000m but risk
is less in Yangon and Mandalay - Regimen 1. (Mefloquine
resistance on Thai border areas).
1
C
R
R
R
R
-
-
L
L
L
Nepal Malaria
risk in areas below 1200 metres e.g. the Chittwan
National Park - Regimen 2. All other areas including
Kathmandu - Regimen 4.
2/4
C
R
R
R
R
R
L
L
L
L
Oman Malaria
risk in remote areas in the north including Musandam
province - regimen 2. Muscat is considered malaria
free.
2
C
R
R
R
R
-
-
L
L
L
Pakistan Malaria
risk is present in the whole country in areas below
2000m (i.e. everywhere except in the Himalayas in
the far north) and more so in the hotter months
and after the monsoon rains (May - October) - Regimen
2.
2
C
R
R
R
R
-
L
L
L
L
COUNTRY
MALARIA
REGIMEN
YEL
HEP
A
TYP
TET
POL
MEN
ENC
DIP
RAB
HEP
B
Philippines Malaria risk present below 600m in rural
areas - Regimen 2.
No risk in the island provinces of Aklan, Bilaran,
Bohol, Camiguin, Catanduanes,
Risk is small in the plains to the north of Manila
and other major cities - Regimen 4.
2/4
C
R
R
R
R
-
L
L
L
L
Qatar No malaria
risk
-
-
R
R
R
R
-
-
L
L
L
Russia No malaria
risk
-
-
R
R
R
R
-
-
R
L
L
Saudi
Arabia Malaria
risk exists throughout the year in most of the Southern
Region and in certain rural areas of the Western
region - Regimen 2.
No risk in Mecca or Medina or in the high altitude
areas of Asir Province - Regimen 4.
*meningococcal
vaccination is now mandatory for pilgrims on Hajj
to Mecca, otherwise recommended for stays of one
month or more.
2/4
C
R
R
R
R
R
M*
-
L
L
L
Singapore No malaria
risk.
-
C
R
R
R
R
-
-
L
-
L
Sri
Lanka Malaria
risk in the whole country - Regimen 2.
Colombo and the coastal resorts of Galle, Nuwara
Eliya and Kalutara, no risk of malaria but bite
avoidance is recommended - Regimen 4.
2/4
C
R
R
R
R
-
L
L
L
L
Syria Malaria
risk exists in northern border areas from May to
October.
3
C
R
R
R
R
-
-
L
L
L
Taiwan No malaria
risk
-
-
R
R
R
R
-
-
L
L
L
Tajikistan Malaria
risk exists from June - October, particularly in
southern border areas (Khatlon region) and in some
central (Dushanbe), western (Gorno-Badakhshan),
and northern (Leninabad) areas.
3
-
R
R
R
R
-
-
L
L
L
Thailand Malaria
risk is present throughout the year but mainly
in rural and forested areas near the borders with
Myanmar (Burma), Laos and Cambodia - Regimen 1.
Since mefloquine resistance is now common in these
areas, Malarone OR doxycycline is usually advised.
The risk is virtually non esistant in major cities
such as Bangkok, Chiang Mai, Chiang Rai and the
tourist resorts of Pattaya, Phuket, the River
Quai bridge area and the Ko Samui islands - Regimen
4.
There is very little risk in the central parts
of the country and along the coastal road and
train routes from the Malaysian/Thai peninsular
into central Thailand - Regimen 4.
Turkey Risk occurs
from March to November, mainly in the south-eastern
part of the country; Antalya, Side and Alanya, the
east coast, south east Anatolia the plain around
Adona, the Syria and Iraq borders and in Amikova
and Cukurova Plain - Regimen 3
There
is no malaria risk in the main tourist areas in
the west and south-west of the country. No risk
west of Antalya - Regimen 4.
3/4
-
R
R
R
R
-
-
L
L
L
Turkmenistan Malaria
risk in the south-east, mainly Mary district, from
June-October.
3
-
R
R
R
R
-
-
L
L
L
United
Arab Emirates There
is a very limited malaria risk in some valleys in
the east and in the northern rural areas of the
country - Regimen 2.
There is not normally any risk in Abu Dhabi and
the cities of Dubai, Sharjah, Ajman and Umm al Qaiwainrisk
- Regimen 4.
2/4
-
R
R
R
R
-
-
L
L
L
Uzbekistan No malaria
risk
-
-
R
R
R
R
-
-
L
L
L
Vietnam Malaria
risk is present in the whole country - Regimen 1.
Excluding urban centres such as Ho Chi Min City
(Saigon) and Hanoi, the Red River delta and the
coastal plain areas of central Vietnam north of
Nha Trang - Regimen 4.
1/4
C
R
R
R
R
-
L
L
L
L
Yemen Malaria risk
exists throughout the year but mainly from September
to February, in the whole country below 2000m. Malaria
risk on Socotra Island - Regimen 2.
There is no risk in Sana'a city. In Aden and the
airport perimeter the risk is minimal - Regimen
4.
2/4
-
R
R
R
R
-
-
L
L
L
The information supplied
here is derived from a number of reliable
sources and is compared and compiled into the
alphabetical lists found on this web site.
Countries requiring malaria prophylaxis should
be regarded as being at risk all year round
and you should also assume that the whole country
is at risk unless otherwise indicated. Themalaria regimen is therecommended
regimen for a country. Use of the incorrect regimen
may not provide adequate cover.
When there are two different regimens
for the same country, they are area specific.
Read the text to find out which regimen is suitable
for the area you require.
Where regimen 1 is indicated there is Chloroquine
resistance in that region and it is very likely
to be the Falciparum malaria which is the most
serious form of the disease. In this instance
it is vitally important that travellers take adequate
prophylaxis.
Remember:-No prophylaxis is 100% effective
but not taking anti-malarials where they are indicated
will put you at greater risk should you get the
disease. Remember - Malaria is a killer!
The Different Drug Regimens
Regimen
1
Mefloquine one 250mg tabletweekly. OR
Doxycycline one 100mg capsule daily. OR
Malarone one tablet daily.
No
prophylactic tablets required but anti mosquito measures
should be strictly observed: Avoid
mosquito bites by covering up with clothing such as long
sleeves and long trousers especially after sunset, using
insect repellents on exposed skin and, when necessary,
sleeping under a mosquito net.
.
Proguanil
100mg tablets are
supplied as Paludrine Tablets
Chloroquine
150mg tablets are
supplied as Nivaquine or Avloclor Tablets
Mefloquine
250mg tablets are
supplied as Lariam Tablets
Malarone
is a
combination of Atovaquone 250mg and Proguanil
100mg
Length of Prophylaxis
Chloroquine, Proguanil & Maloprim
Start
one week before travel, throughout your stay in
an endemic area and continue for four weeks after
return.
Mefloquine (Lariam)
Start
two and a half weeks before travel, throughout
your stay in an endemic area and continue for four
weeks after return.
Doxycycline
Start two days before travel, throughout
your stay in an endemic area and continue for four
weeks after return.
Malarone
Start
two days before travel, throughout your stay in
an endemic area and continue for one week after
return.
IMPORTANT!
Take the
tablets absolutely regularly, preferably with or after
a meal.
Long Term
Use of Anti-Malaria Drugs
Chloroquine
May be
taken for periods exceeding five years.
Paludrine
May be
taken for periods exceeding five years.
Maloprim
Can be
taken for periods up to one year.
Mefloquine
Can be
taken for periods up to one year.
Doxycycline
Can be
taken for periods up to six months.
Malarone
Can be
used for travel periods up to one year.
Compatibility of Anti-Malaria Drugs
Pregnancy
Breast
Feeding
Epilepsy
Psoriasis
Altitude
Scuba
Diving
Chloroquine
OK
OK
NO
NO
OK
OK
Paludrine
OK
OK
OK
OK
OK
OK
Mefloquine
OK*
NO
NO
OK
NO
NO
Doxycycline
NO
NO
OK
OK
OK
OK
Malarone
NO
NO
OK
OK
OK
OK
*
These drugs are not suitable during the first trimester
of pregnancy.
Childrens' Dosages: Calculate
the dose by weight rather than by age if possible
Age/Weight
Chloroquine
(once weekly)
Proguanil
(once daily)
Mefloquine
(once weekly)
Doxycycline
(once daily)
Malarone
(once daily)
0
- 12 weeks
under 6kg
1/4
tablet
1/4
tablet
-
-
-
3
- 12 months
6 - 10kg
1/2
tablet
1/2
tablet
1/4
tablet
-
-
1
- 3 years
10 - 16kg
3/4
tablet
3/4
tablet
1/4
tablet
-
1
child's
tablet
4
- 7 years
16 - 25kg
1
tablet
1
tablet
1/2
tablet
-
1
child's
tablet
8
- 12 years
25 - 45 Kg
11/2
tablets
11/2
tablets
3/4
tablet
-
2
child's
tablets
13
years and over
45kg and over
2
tablets
2
tablets
1
tablet
1
capsule
1
adult
tablet
The
above dosages are based upon the guidelines issued by
the Advisory Committee on Malaria Prevention.
Adult
Dosages
Regimen
Dose
for
Chemoprophylaxis
Usual
amount
per tablet (mg)
Areas
without drug resistance:
Chloroquine
Proguanil
2
tablets weekly
2
tablets daily
150mg
(base)
100mg
Areas
of little chloroquine resistance (poorly effective where
marked resistance):
Malaria
prevention guidelines for travellers to Goa
In
early 2007 a number of cases of Plasmodium falciparum
malaria were reported in UK travellers returning
from Goa. None were known to have taken malaria
chemoprophylaxis. During the same period, a number
of cases were also seen in other European travellers.
This has resulted in the guidelines being revised
to recommending chemoprophylaxis for all travellers
visiting Goa.
The
current recommendations for travellers visiting
Goa are as follows:
Malaria
chemoprophylaxis is recommended to those travellers
who will be visiting Goa , particularly areas
north of Panaji. The recommended chemoprophylaxis
is chloroquine plus proguanil. Alternatives are
mefloquine, Malarone, or doxycycline.
All travellers to Goa should also use mosquito
bite avoidance measures.
All
travellers should seek medical attention promptly
if they become unwell whilst away or after returning
and inform their doctor that they have been in
a malarious area. The healthcare worker should
consider malaria in every ill patient who has
recently returned from the tropics; for those
with a fever, the illness should be considered
to be malaria until proven otherwise.